Δημοσιεύσεις
Μερικά άρθρα σε επιστημονικά περιοδικά.
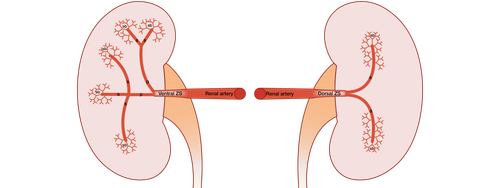
Anatomical Variability of Kidney Arterial Vasculature Based on Zonal and Segmental Topography
To date, there is no unified approach to the lobar, zonal, and segmental structure of the kidney vasculature. There is no recognizable approach to define basic characteristics in regard to the lobes and segments identifying of the kidney. The branching of the renal artery has often been the subject of scientific research. This study aimed to analyze the arterial anatomy on the basis of zonal and segmental topography. This study is a prospective cadaver study on autopsy material using corrosion casting and CT imaging techniques. The arterial vasculature was visualized using corrosive casting. In this study, 116 vascular casts were included. We identified the number of arteries in the kidney hilum, their topography, branching variations of the renal artery, and local blood supply zones of renal masses considering second- and third-order renal artery branches. We used a micro-CT BRUKER SkyScan 1178, digital camera, Mimics-8.1, and R. This study has shown that RA divides into two or three zonal arteries, forming a two- or three-zonal vascular supply system. In the case of the two-zonal system, 54.3% of cases accounted for RA branching into ventral and dorsal arteries, whereas 15.5% of cases referred to superior polar and inferior polar zonal arteries. The three-zonal system implies 4 types of RA branching: 1) superior polar, ventral, and dorsal zonal branches (12.9%); 2) ventral, dorsal, and inferior polar zonal branches (9.5%); 3) two ventral and one dorsal zonal branches (5.2%), and 4) superior polar, central, and inferior polar zonal branches (2.5%). The results of this research make us reconsider Graves' classification theory.
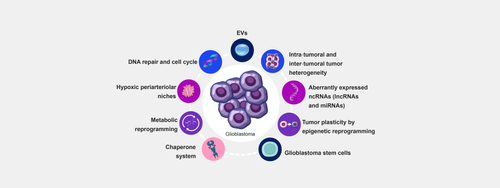
Molecular Pathways Implicated in Radioresistance of Glioblastoma Multiforme: What Is the Role of Extracellular Vesicles?
Glioblastoma multiforme (GBM) is a primary brain tumor that is very aggressive, resistant to treatment, and characterized by a high degree of anaplasia and proliferation. Routine treatment includes ablative surgery, chemotherapy, and radiotherapy. However, GMB rapidly relapses and develops radioresistance. Here, we briefly review the mechanisms underpinning radioresistance and discuss research to stop it and install anti-tumor defenses. Factors that participate in radioresistance are varied and include stem cells, tumor heterogeneity, tumor microenvironment, hypoxia, metabolic reprogramming, the chaperone system, non-coding RNAs, DNA repair, and extracellular vesicles (EVs). We direct our attention toward EVs because they are emerging as promising candidates as diagnostic and prognostication tools and as the basis for developing nanodevices for delivering anti-cancer agents directly into the tumor mass. EVs are relatively easy to obtain and manipulate to endow them with the desired anti-cancer properties and to administer them using minimally invasive procedures. Thus, isolating EVs from a GBM patient, supplying them with the necessary anti-cancer agent and the capability of recognizing a specified tissue-cell target, and reinjecting them into the original donor appears, at this time, as a reachable objective of personalized medicine.